SCOPE
Quick Facts
 Provinces
Provinces
Alberta and British Columbia
 Type of study
Type of study
Randomized control trial (RCT)
 Facilities involved
Facilities involved
14 facilities in Alberta
17 facilities in British Columbia
 Target audience
Target audience
Care aides
LTC facility management
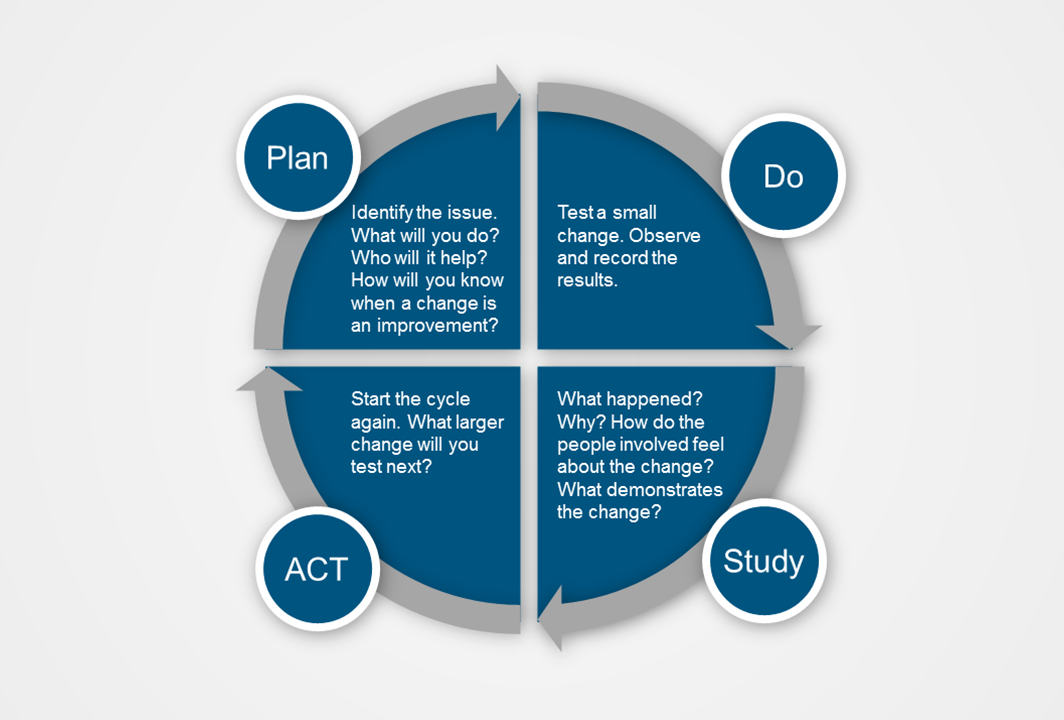
What is Involved?
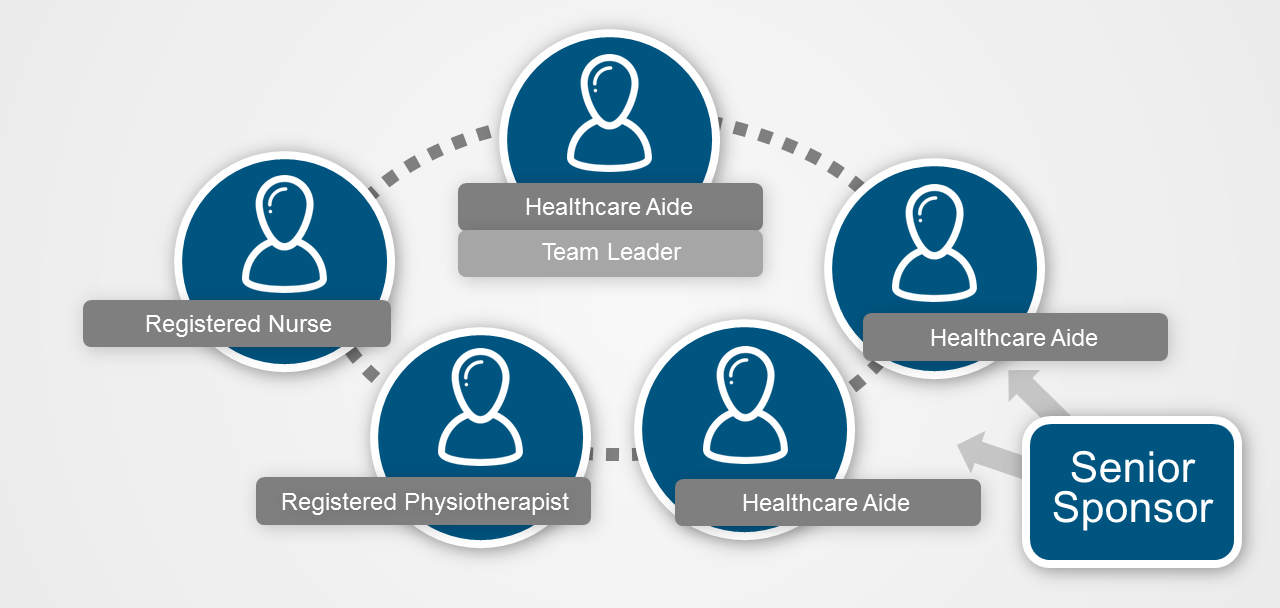
Teams of five staff members on one unit within a participating nursing home initiated and tested the effect of quality improvement activities in their daily delivery of care. The teams were made up of 3 Care Aides (one of whom led the team) and 2 other members of staff, with support from a Team Sponsor and a Senior Sponsor. Each team chose to focus on one of three areas: recognizing and treating pain, optimizing resident mobility or accommodating dementia-related responsive behaviour.
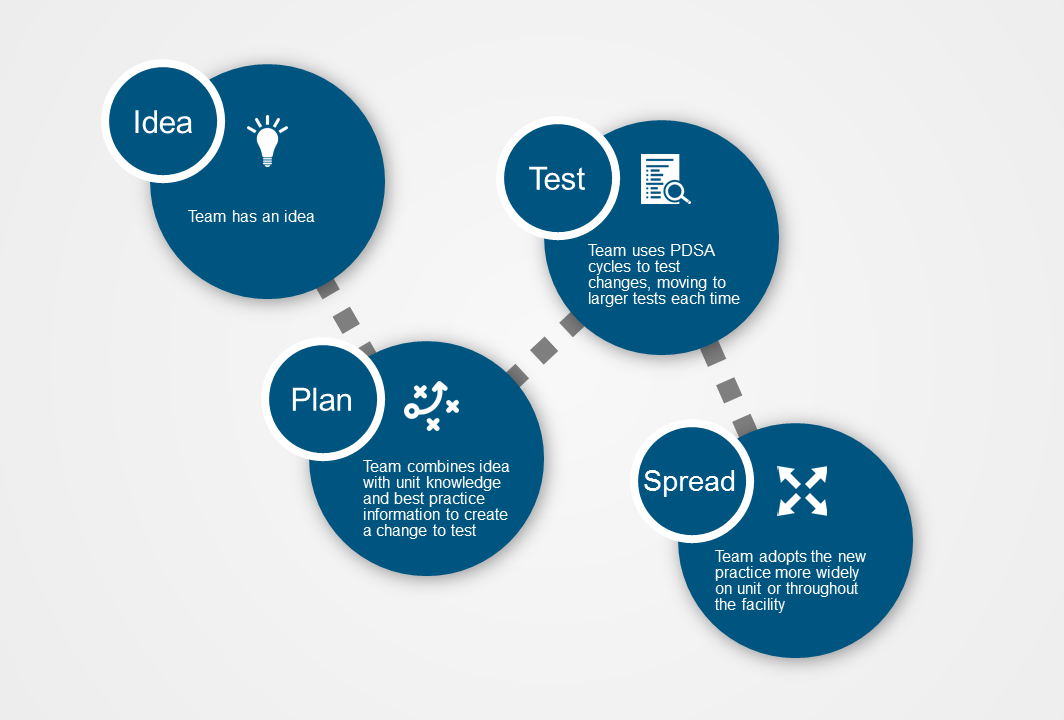
Throughout the year that the intervention took place, teams received regular coaching from the SCOPE Quality Advisor and participated in monthly teleconferences. They also attended four Learning Congresses - events that brought together all teams to participate in educational sessions, and share their challenges.
Quality Improvement Team
Page Options


